Fracture NOF Case Presentation
CASE PRESENTATION
INTRODUCTION:
Fracture
of the neck of the femur is an important injury for many reasons.
Ø It is common and the incidence is increasing.
Ø It is not always easy to diagnose.
Ø Fractures can occur in all age groups but the majority
of are caused by falls in the elderly and the fracture usually occurs through
osteoporotic bone. An understanding of fractured neck of femur requires an
understanding of falls and osteoporosis. (women > men)
Ø Patients with this injury often have many
co-morbidities and the fracture has a substantial mortality rate. Management of
this injury is often used as a model for management of acute problems in the
elderly.
Ø Pathophysiology
ü healing
potential
§ femoral
neck is intracapsular, bathed in synovial fluid
§ lacks
periosteal layer
§ callus
formation limited, which affects healing
Ø Associated
injuries
ü femoral
shaft fractures
§ 6-9%
associated with femoral neck fractures
§ treat
femoral neck first followed by shaft
Ø Prognosis
ü mortality
§ ~25-30%
at one year (higher than vertebral compression fractures)
ü predictors
of mortality
§ pre-injury
mobility is the most significant determinant for post-operative survival
§ in
patients with chronic renal failure, rates of mortality at 2 years postoperatively,
are close to 45%
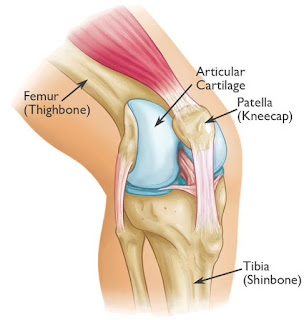
ANATOMY:

CLASSIFICATION:
GARDEN
CLASSIFICATION:

PAUWELS CLASSIFICATION:

PATIENT INFORMATION:
Ø Patient
Name: “ X”
Ø Age:
83yrs/Female.
Ø Date
of Admission: 21/11/2018.
Ø Date
of Surgery: 28/11/2018.
CHIEF COMPLAINT:
Patient had pain over the left hip joint, restricted left hip movements and
inability to stand and walk few steps since today (21/11/2018).
HISTORY OF PRESENT ILLNESS:
Patient came with complaints of pain over the
left hip, deformity over the left hip and was unable to stand and walk few
steps since today (21/11/2018). Patient gave history of slip and fall at
bathroom (at home) today (21/11/2018). Since then patient complaints of pain,
swelling, deformity and inability to use left hip (left thigh region). After
the injury patient came to emergency department of our hospital.
v Previous
Injury: Fracture neck of femur right side in the year
2007
v Developmental
History: No any developmental histories
v Drug
History: No known drug allergies. Not on any chronic
medication
v Past
medical History: No Diabetes Mellitus; No Hypertension; No
Bronchial Asthma;No Thyroid diseases.
ON EXAMINATION:
Patient is conscious, oriented.
Vital Signs:
· BP
– 130/70 mm/Hg
· PR
– 78 b/min
· SpO2
– 98%
· Temp
– 99° F
LOCAL EXAMINATION:
Ø Pain
and swelling over the left hip and thigh are present.
Ø Tenderness
and crepitus over the left hip are present.
Ø Deformity
and angulation over the left hip are present.
Ø Any
attempted movements of the left hip are painful.
Ø Distal
pulse palpable (A. Dorsalis Pedis).
X-RAY FINDING:
NORMAL PELVIS

Patient X-ray Findings:

Ø CT
·
helpful in determining displacement and degree of comminution in some
patients
- MRI
·
helpful to rule out occult fracture
·
not helpful in reliably assessing viability of femoral head after fracture
PREPARATION:
Preoperative
planning
Whatever
arthroplasty is chosen, the procedure should be carefully planned with
sufficient detail. Select the prosthesis with the aid of radiographic templates
(or electronic planning software with digital x-rays) and appropriate
x-rays of the normal and injured hip.
In addition to the selected prosthesis, possible alternatives should be available in the operating room.
In addition to the selected prosthesis, possible alternatives should be available in the operating room.

Lateral decubitus position
The patient
is positioned lateral with the ipsilateral arm in arm sling. Place padded
cushions under bony prominences to avoid excessive pressure.

SKIN INCISION:
Anterolateral approach:
Start the slightly anteriorly curved skin incision about 7-10 cm
proximal of the lateral part of the greater trochanter (directed towards the
tubercle of the iliac crest – the posterior landmark of tensor fascia lata
origin). Distally, the incision extends along the femur about 10 cm below the
greater trochanter.

Opening of the joint capsule
Make a
T-shaped incision in the capsule

Removal of femoral head:

Post
Operation X-ray:

CLASSIFICATION:
According to the classification. The fracture is classified:
Ø
Garden type IV: Complete fracture, completely displaced.


Ø
Simplified Garden: Displaced.
Ø
Pauwels type III: >50 degree from horizontal (most
unstable and high risk of non-union and AVN).
CONCLUSION:
Ø Early surgery, good anatomical
reduction and internal fixation help to recover the full range of movements.
Ø Stability has been RESTORED.
--THE END--


Comments
Post a Comment
Thank you for your kind words and your support.