CONGENITAL SYNOSTOSIS
CONGENITAL
RADIAL-ULNAR SYNOSTOSIS
INTRODUCTION:
Synostosis, or osseous
union, of any two adjacent bones can involve any part of the upper extremity. In 1793, Sandifort provided the initial description of congenital radial-ulna synositis. This condition is caused by a
failure of segmentation between the radius and the ulna. Synositis between the radius and ulna can take two general forms: Congenital and post-traumatic
v Forearm begins as a single cartilaginous and divides from distal to proximal into the radius and ulna in the 7th week in utero.
v Failure of differentiation results in synostosis in proximal aspect of the forearm.
v 60% of the cases are BILATERAL.
v Male
are more affected than Female (3:2)
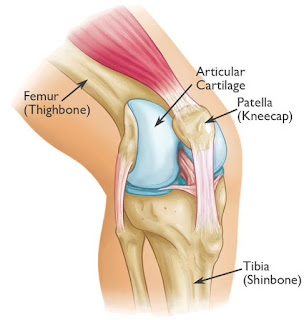
ANATOMY;


SIGNS AND SYMPTOMS:
Ø Painless
Ø Most
commonly asymptomatic, noticed by parents and teachers.
Ø Can
notice or identify difficulty with specific movements/tasks
v Keyboard,
table-top activities – Deficient Pronation.
v Eating,
washing face, catching a ball – Deficient Supination.
CLASSIFICATION:
Wilkie divided congenital synostosis
into the following two types on the basis of the proximal radio-ulnar junction:
Ø Type 1 - Complete synostosis has
occurred, with the radius and ulna fused proximally for a variable distance
Ø Type 2 - Less involved, and may exist
as a partial union; this type involves the region just distal to the proximal
radial epiphysis and is associated with radial head dislocation
Cleary and Omer described four
types of congenital synostosis, as follows:
Ø Fibrous synostosis
Ø Bony synostosis
Ø Associated posterior dislocation of the
radius
Ø Associated anterior dislocation of the
radius
Simmons considered
congenital synostosis to be a spectrum of anomalies in which the synostosis
occurred in varying lengths, with or without involvement of the radial head.
EXAMINATION
AND TEST:
Ø Average age of diagnosis is 6 years of age
v Can go unnoticed until early
adolescence, especially in unilateral cases
Ø Elbow flexion usually preserved
Ø Fixed forearm pronation
v Average position is 30° of pronation
Ø Compensatory motion
v Shoulder abduction - compensates for
loss of active pronation
v Shoulder adduction - compensates for
loss of active supination
v Wrist hypermobility.
DIAGNOSTIC METHOD:
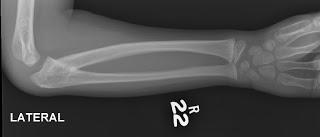
Ø X-ray
Normal x-ray of
elbow:

X-ray changes in Congenital
Radial-Ulna Synosytis:

Ø CT-scan (in rare cases advised)

TREATMENT:
Ø
Non-Surgical Method:
Observation is the preferred treatment,
particularly when asymptomatic and unilateral.
Ø
Surgical Method:
v Indication
is when absolute deformity is limiting ability to participate in specific activities
and movements.
v Surgery
is indicated when relative severe pronation deformity > 60o with bilateral deformities.
v Osteotomy
– to improve static forearm and hand movements.
Doctor decides the treatment according to the severity by monitoring the
changes and type according to the classification.
--THE END--


{kind=link}
Comments
Post a Comment
Thank you for your kind words and your support.